Hypnosis & Applied Relaxation (AR)
January Research Snippet by Donald Robertson, NCH Research Director
(Some of the material for this post is derived from the forthcoming book The Practice of Cognitive-Behavioural Hypnotherapy. Copyright (c) Donald Robertson, 2011. All rights reserved.)
This month’s snippet is a bit of a change again: a slightly longer article providing the whole outline of a modern evidence-based behaviour therapy for anxiety, which is well-suited to be assimilated into hypnotherapy. People often ask “Why isn’t there more research on hypnosis?” In fact, the people who ask this, in my experience, never seem to have read (or even heard of) the main research journals in the field of hypnosis (IJCEH, AJCH, and Contemporary Hypnosis) and are unaware that there’s actually an awful lot of research on hypnosis, arguably more than on any other psychological therapy, apart from cognitive-behavioural therapy (CBT). However, one of the problems facing hypnosis researchers is that methods of hypnotherapy are too messy, eclectic and complex to be well-suited to good research design. It helps build an evidence base if a treatment is “manualised” and can be described in a guide so that other researchers can replicate it in independent studies. Hypnotherapists tend to do lots of strange things with clients, making it difficult to isolate which “bits” are effective and which bits are redundant. Modern research on psychological therapies is constantly evolving and improving in quality. Protocols for therapies tend to have become simpler in order to facilitate the process of research.
A well-known example is the “Applied Relaxation” protocol developed in Sweden by the psychologist Lars-Goran Öst, currently a professor at the University of Stockholm, and his colleagues (Applied Relaxation: Description of a Coping Technique and Review of Controlled Studies, 1987). It developed out of Edmund Jacobson’s Progressive Muscle Relaxation, Wolpe’s Systematic Desensitisation, and a variety of “coping skills” approaches to anxiety management that evolved in the 1970s. The following account is based on Öst’s original protocol and the self-help version published by Davis et al. (Davis, et al., 1995 pp. 65-74; Applied Relaxation: Description of a Coping Technique and Review of Controlled Studies, 1987). Although essentially a form of modern behaviour therapy, Applied Relaxation has also been used in combination with cognitive restructuring as part of a cognitive-behavioural therapy (CBT) approach.
Applied Relaxation is of interest to hypnotherapists because it consists of a very simple treatment protocol employing relaxation coping skills, which has been adapted for use with a range of problems, and supported by a number of well-designed research studies. It has met critical appraisal criteria for being classed as an Empirically-Supported Treatment (EST) for panic disorder and research has also supported its efficacy in the treatment of generalised anxiety disorder (GAD) and, to some extent, for specific phobias, headache, pain, epilepsy, tinnitus, and other conditions. It’s also been recommended for general management of worry and stress, i.e., for subclinical problems.
I think this protocol would be of interest to hypnotherapists because the method closely resembles “hypnotic desensitisation” (Wolberg, 1948; Wolpe, 1958) and it provides a good example of how a simplified hypnotherapy treatment protocol could be developed for use in treatment outcome research. When reading the description below, just consider replacing the Jacobson tension-release relaxation method with self-hypnosis training in suggested relaxation and (I hope) it should be easy for hypnotherapists to see how this coping skills framework can be directly modified and transformed into a simple behavioural hypnotherapy method for anxiety.
Overview of the Applied Relaxation (AR) Protocol
The full text of a journal original article by Prof. Öst describing the method in detail is currently available online at this link.
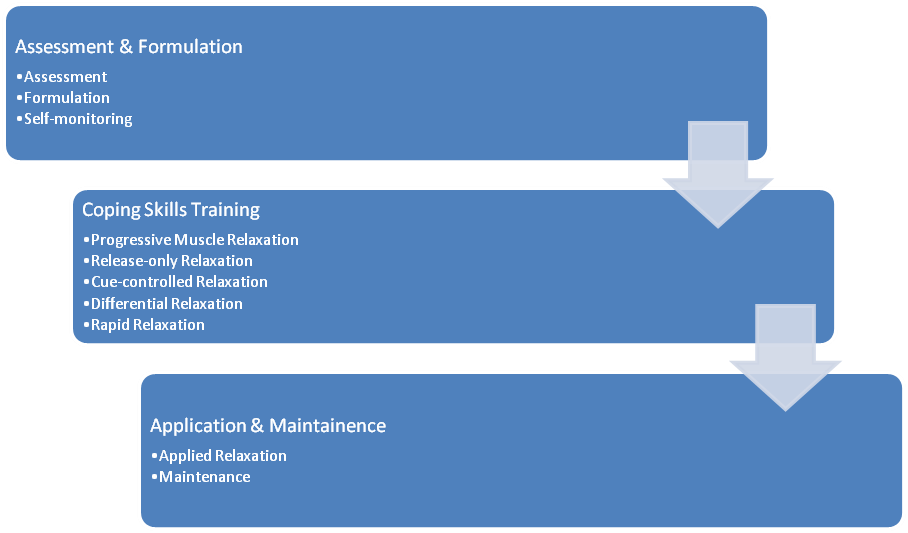
In brief, Applied Relaxation begins with training in Progressive Muscle Relaxation, which is gradually developed into a cue-controlled relaxation coping skill, and systematically applied during in vivo exposure to feared situations. The original protocol takes about 10-12 sessions, following assessment, and the specific stages of treatment are as follows,
- Assessment, formulation, and self-monitoring, which Öst seems to imply takes 2-3 sessions prior to training
- Progressive Muscle Relaxation, lasting 2-3 weeks/sessions
- Release-only relaxation, lasting 1-2 weeks/sessions
- Cue-controlled relaxation, lasting 1-2 weeks/sessions
- Differential relaxation, lasting 1-2 weeks/sessions
- Rapid relaxation, lasting 1-2 weeks/sessions
- Applied relaxation (application training), lasting 2-3 weeks/sessions
- Maintenance
1. Assessment & Formulation Phase
The full protocol begins with behavioural analysis and self-monitoring, usually carried out over three weeks. Clients are asked to begin during the first week by recording their experiences on a very simple self-monitoring form that contains the following three headings: Date, Situation, and Intensity (rated 0-10). In the second week, a column is added headed “Reaction (What did you feel?)”, and finally, in the third week, a column is included headed “Action (What did you do?”). The final self-monitoring form, therefore contains headings as follows,
| Tension Self-Monitoring Record | ||||
|
Date/Time |
Situation |
Reaction (What did you feel? Focus on the earliest signs.) |
Intensity (0-100%) |
Action (What did you do?) |
Öst introduces clients to a three-system conceptualisation model of anxiety (or stress) that distinguishes between physiological sensations, behaviour, and cognitive (subjective) responses. The emphasis of assessment and conceptualisation is on helping the client spot the signs of stress, especially the earliest stages of the response developing. This tends to particularly involve identifying common physiological sensations, such as muscles tensing or heart rate increasing, and environmental antecedents such as typical events or situations that are associated with elevated stress. Öst recommends presenting the treatment rationale to clients as follows,
One good way of breaking this development [of anxiety] is to focus on the physiological reactions and learn not to react so strongly. The method we are going to use to achieve this is called applied relaxation. The aim of this technique is to learn a skill of relaxation, which can be applied very rapidly and in practically any situation. This skill can be compared to any other skill, e.g. learning to swim, ride a bike, or drive a car, in that it takes time and practice to learn, but once you have mastered it you can use it anywhere. You are not restricted to the calm and non-stressful situation in my office or your own home. The goal is to be able to relax in 20-30 sec and to use this skill to counteract, and eventually get rid of, the physiological reactions you usually experience in phobic situations. To achieve this we are going through a gradual process starting with tensing and relaxing different muscle groups. This takes about 15 min, and you are to practice it twice a day. Then we start to reduce it by taking the tension part away, just relaxing, which takes 5-7 min. The next step teaches you to connect the self-instruction “Relax” to the bodily state of relaxation. Then we teach you to do different things while still being relaxed in the rest of your body, and also relaxing while standing and walking. After that it is time for the rapid relaxation, which you practice many times a day in non-stressful situations. Finally, you reach the stage of applying the skill in phobic situations, and I will take you to different anxiety arousing situations coaching you how to apply the relaxation at the first signs of anxiety in these situations. Applied relaxation is thus a skill that most people can acquire with the right instructions and a lot of practice. It is a “portable” skill that can be used in almost any situation and is not restricted to phobias, but can be used in other situations, e.g. when having problems in falling asleep. (Applied Relaxation: Description of a Coping Technique and Review of Controlled Studies, 1987)
2. Coping Skills Training Phase
2.1 Progressive Muscle Relaxation
The first phase of actual Applied Relaxation training consists of Jacobson’s Progressive Muscle Relaxation technique, which Öst derives directly from the abbreviated approach introduced by Wolpe and Lazarus as part of Systematic Desensitisation (Wolpe, et al., 1966; Jacobson, 1938). This training is divided across the first 2-3 sessions, the first of which focuses on relaxing the head and arms (hands, arms, face, neck, and shoulders), to which are added, in the second session, relaxation of the torso and lower body (back, chest, stomach, breathing, hips, legs, and feet). In Öst’s version, each muscle group is tensed for only five seconds, much abbreviated from Jacobson’s original method, followed by 10-15 seconds of relaxation. In Jacobson’s original approach, the aim is to learn to keep relaxing the rest of the body while tensing individual muscle groups, i.e., to only tense the muscles you’re deliberately using, which helps create a bridge to the “differential relaxation” stage (Jacobson, 1938). At the end of the procedure, the client rates their level of tension on scale (0-100%), similar to a traditional SUD scale, where zero means absolute relaxation and 100% means maximum tension – the same self-rating scale used during homework. Although people do normally find it easier to relax when lying down, training begins in a seated upright position, as the purpose is to develop a coping skill that will generalise to situations where the client is physically active. The same relaxation routine is to be practised twice daily for homework, sessions typically lasting about 15-20 minutes, with each recorded on a homework form for review during sessions.
| Relaxation Homework Record | |||||
| Date/Time | Component(Technique) | Tension Before(0-100%) | Tension After(0-100%) | Duration(Minutes) | Comments(Any difficulties?) |
2.2 Release-only Relaxation
The next phase of Applied Relaxation, like the original Progressive Muscle Relaxation approach, focuses on “release-only relaxation” training for an additional 1-2 weeks. In this phase, the initial tensing of muscles is omitted, some basic skill having been acquired in closely studying the contrasting sensations of tension and relaxation. This also means a reduction in the time taken to induce relaxation from 15-20 minutes to 5-7 minutes. The therapist verbally prompts the client to “Breathe with calm, regular breaths and feel how you relax more and more for every breath… Just let go… Relax your forehead… eyebrows… eyelids… jaws… tongue and throat… lips… your entire face…”, etc. (Applied Relaxation: Description of a Coping Technique and Review of Controlled Studies, 1987). The client then scans their body for any remaining tension and tries to relax completely. However, if the client does find tension creeping back into a muscle group during release-only relaxation they are to revert to the original tension-release technique, for that part of the body alone.
2.3 Cue-controlled Relaxation
The next phase, cue-controlled relaxation, involves training in a “verbal cue” or “self-instruction” to induce relaxation more quickly, usually in around 2-3 minutes, by using the word “RELAX”, which is practised for another 1-2 weeks. This is apparently conceptualised by Öst as a process of conditioning the relaxation response to the verbal stimulus (“RELAX”). During the session the client relaxes as deeply as possible using the release-only approach, signalling when they have done so by raising a finger. The client then focuses on their breathing, while the therapist repeatedly says the words “INHALE”, just before each inhalation, and “EXHALE”, before each exhalation, five times in a row. The therapist then fades this verbal prompt and the client takes over using her own self-instruction by saying “INHALE” and “RELAX” internally (covertly), in a similar manner. After about a minute, the therapist begins repeating the words again, about five times, and the client takes over again, repeating the process above, and once more after a break of about fifteen minutes. The therapist should ask the client to estimate how long it took them to relax completely, and feedback the correct answer, because, as Öst points out, clients typically over-estimate the duration. This routine should also be practised about twice per day, to help condition an association between the verbal cue “RELAX” and rapid release-only relaxation.
2.4 Differential Relaxation
The next phase involves “differential relaxation, again derived from Jacobson’s approach, which consists of learning to relax while using some muscles. The client is asked to induce cue-controlled relaxation while seated in a hard chair or standing, and to remain relaxed while moving their head or arms, or legs, etc., and finally while walking. Emphasis is placed on further reducing the time taken to induce relaxation, which typically comes down to 60-90 seconds, according to Öst.
2.5. Rapid Relaxation
This is followed by a “rapid relaxation” training phase, which aims to help the client relax in vivo, in naturally stressful situations, while further reducing the time taken for relaxation to 20-30 seconds. The client is asked to relax 15-20 times each day for homework. Obviously, this means the technique is used very frequently throughout the day, and so cues are identified to act as reminders, such as each time the client checks the time on a watch or clock, or opens a door, etc. Sticky notes or other reminders can be used in the work or home environment to act as additional reminders. The rapid form of cue-controlled relaxation consists in taking three deep breaths, saying “RELAX” internally after each one, before exhaling slowly. The body is then scanned for any remaining tension, and the client tries to maintain maximum relaxation in the real-world situation.
3. Application & Maintanence Phase
3.1 Application
The “application” phase usually begins after roughly 8-10 sessions of preceding training, and involves brief exposure to a wide variety of anxiety-provoking stimuli and situations. The client is encouraged to use their cue-controlled relaxation coping skill immediately prior to exposure, and to continue to use the technique during exposure, in response to any initial signs of escalating tension. Exposure using Applied Relaxation typically takes 10-15 minutes, much briefer than normal prolonged exposure sessions, which can last 1-2 hours. However, the aim is not to extinguish anxiety completely but rather to learn to cope with it by using cue-controlled relaxation as a coping strategy. The client may be exposed in vivo to feared objects or events, or through interoceptive exposure to panic sensations, or using imaginal exposure, especially for feared catastrophes in worry and GAD.
3.2 Maintanence
Training is followed by a “maintenance” programme to help ensure that the coping skill further generalises to different situations in the future and is not simply forgotten. To help maintain the skill, clients are asked to scan their body at least once each day and use their rapid relaxation method to dispel any tension identified, and to practice either differential or rapid relaxation at least twice per week. The client may also keep the therapist updated by posting them records of their progress, e.g., for a period of six months after treatment.
Hypnosis & Applied Relaxation
Very little in Öst’s original protocol needs to be changed in order, I think, to legitimately transform it into a hypnotherapy technique. As cognitive-behavioural approaches to hypnotherapy typically conceptualise hypnosis mainly as a form of self-hypnosis, and emphasise specific evidence-based skills training procedures (such as Nicholas Spanos‘ CSTP), cognitive-behavioural hypnotherapy in particular lends itself well to a “coping skills” approach, like Öst’s Applied Relaxation. There’s not much reason to believe that the tension-release (Jacobson) method has significant advantages in relation to treating common problems over suggestive methods like Autogenic Training, which can easily be used instead as part of a hypnotic version of Applied Relaxation.


